")
Continence is the ability to exercise voluntary control over the bowel and bladder. Many people with Spina Bifida are incontinent, that is, they are unable to control their bowel and bladder discharge resulting in involuntary loss of urine (urinary incontinence) or faeces (faecal incontinence).
People with Spina Bifida generally have what is termed a “neurogenic bladder and bowel” which means that there has been an interruption to the communication between the nerves of the spinal cord and the bladder and bowel. This results in the brain not being able to control the muscles that coordinate bladder and bowel function.
What happens if continence is not well managed?
Possible health impacts:
- Not managing bowel continence issues can lead to an overloaded bowel. This can result in kidney damage, UTIs, and can cause the bowel to become obstructed, which may be a life-threatening emergency. Episodes of ‘overflow’ (bouts of uncontrollable, explosive ‘diarrhoea’) is caused by chronic overloading and is treated by clearing out the bowel.
- Not managing bladder continence can lead to urinary tract infections and if ongoing, to kidney failure – refer to the Kidney Health information sheet.
- Being wet or soiled is linked to skin problems, particularly it can make you more prone to pressure wounds.
Possible social impacts:
- If you have lived with urinary and or faecal incontinence issues for all of your life, you are often less aware of “accidents”. Those around you, however, are most likely very aware. Incontinence can limit your ability to make friendships, engage in work or any other social activity.
- Complications with sexual activity.
Options for managing urinary incontinence
Urostomy
Common management option prior to the 1970s. A urostomy is a surgical procedure that creates a stoma (artificial opening) for the urinary system. The stoma is generally created in the abdominal wall and it allow urine to pass directly into a collection pouch.
Clean Intermittent Catheterisation (CIC)
Common management option from the 1970s onwards. This option involves passing a catheter directly into the bladder at regular intervals to allow for the drainage of urine. The catheter can be inserted through the urether or through a created stoma.
Continence pads
Pads worn in the underwear are often used by people to manage the leakage of urine, either between catheterisations or if they manage their toileting normally but have occasional incontinence due to urgency.
Bladder augmentation
A surgical procedure which increases the size of the bladder by surgically attaching a portion of bowel to the bladder. By increasing the size of the bladder, its capacity to hold urine is increased. People usually continue to use CIC in conjunction with this procedure.
Artificial sphincter
An artificial sphincter is a device which consists of three main parts – a fluid filled cuff, a pump and a small balloon reservoir. The cuff is placed around the urethra to act like a muscle and control the flow of urine from the body. The artificial sphincter is inserted surgically. The cuff is released by pressing the pump which sits in the scrotum for the male and in the labia for the female. The fluid then moves from the cuff into the balloon reservoir. This is just like releasing your muscle. A catheter is then inserted and urine can flow out. The fluid from the reservoir slowly flows back into the cuff to tighten the urethra again. This allows you enough time to do your catheter before the cuff is tightened again.
Mitrofanoff procedure also known as stoma procedure or Yang procedure
A surgical procedure to create a passage from the bladder to the outside wall of the abdomen to allow for drainage of urine. Catheterisation is then done directly through the stoma in the abdomen wall. This procedure is particularly useful for those people who find it difficult to reach to complete direct urethral catheterisation.
Options for managing bowel incontinence
Regular toilet routine
Use of enemas
MACE procedure (Mitrofanoff Antegrade Colonic Enema) or Malone procedure
Surgical procedure which creates a passage from the top part of your bowel to the wall of the abdomen. This allows for an enema solution to be placed through the stoma into your bowel to thoroughly wash out the bowel from the top downwards.
Anal irrigation (such as the Peristeen system)
System of emptying the lower part of the bowel by slowly introducing warm tap water into the rectum. A catheter is inserted into the rectum and held in place by a balloon. A hand held pump pushes water through the catheter into the bowel. When the balloon is deflated and the catheter removed, the contents of the bowel are discharged.
Being prepared
Plan ahead
Check toilet locations – are there accessible toilets available? There is an app available that shows nearby locations with accessible toilets. Use toilets when you have a chance – even if this means going before your scheduled time.
Check your bag
Have you got enough catheters, pads, undies and change of clothing, medications, deodorant or powder, a plastic bag for wet or soiled clothes?
Continence equipment
In Queensland, there are two types of subsidies available for continence supplies:
- Medical Aids Subsidy Scheme (MASS) – a state government scheme that subsidises the cost of continence aids. Applications can be made with assistance of a Registered Nurse or Occupational Therapist
- Continence Aids Payment Scheme (CAPS) – an Australian government scheme that provides a payment to assist eligible people who have permanent and severe incontinence to meet some of the cost of their continence products.
Toileting for children with Spina bifida
The bladder
The urinary system is one of the most vital systems in the human body. It has two functions: to filter toxic waste and excess water from our blood to form urine, and to return salt and other important elements to the blood. The system, which is made up of two kidneys, two ureters, a bladder, and a urethra, keeps an even balance between water and electrolytes in the body. It is important that this balance is maintained, so it is very important to your child’s health that the urinary system functions properly.
How the urinary system works
The main parts of the urinary system are:
- Kidneys – Two complex organs that filter and process the blood within the body continuously. They filter out the waste products no longer needed by the body, and combine them with water to form urine.
- Ureters – Two thin tubes that channel the urine from the kidneys to the bladder. Each ureter has a small flap of skin at the end of it that closes to prevent urine from flowing backwards up the ureters and into the kidneys.
- Bladder – A muscle lined storage sac for the urine. The bladder stretches to a greater volume as it fills with urine. When the bladder becomes full, sensory receptors alert the brain, which then sends a message to the bladder muscles to contract. When the bladder contracts through controlled movements, pressure builds up and the urine pushes out towards the urethra.
- Urethra – A single tube that enables the passage of urine from the bladder to the outside of the body.
- Urethral Sphincter – Around the top of the urethra are circular muscles called the urethral sphincters. These are voluntary muscles and can be tightened to hold the urine in, or relaxed to allow the urine to empty from the bladder and thus leave the body. This is what allows a person to choose when to urinate.
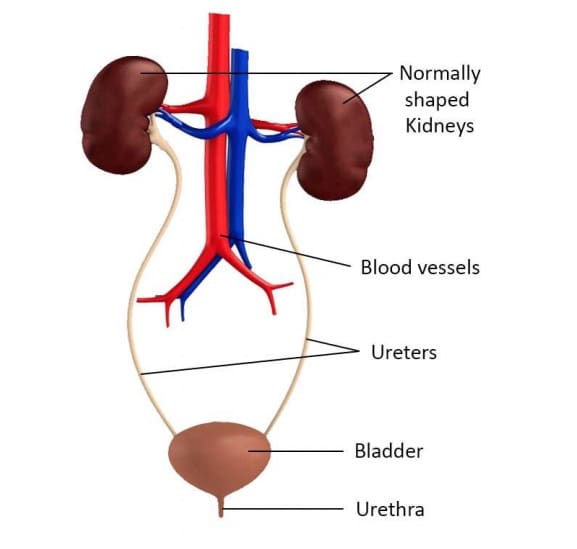
Diagram of a normal urinary system
The bladder is a muscle lined sac. The muscle, called the detrusor, remains relaxed creating a low-pressure reservoir for the urine until urination occurs. A 12-year old’s bladder capacity is about 300-400 mL. A 3- or 4-year-old’s is about half this. The outlet from the bladder is a small tube called the urethra. It is longer in boys than girls, because it passes through the penis. The urethra is surrounded by 2 small circular muscles called sphincters, which remain contracted until urination. One of these operates involuntarily, and the other voluntarily, ie. we can control it.
When the bladder is full sensory receptors tell the brain via the nerves in the spinal cord that the bladder needs emptying. When the person is ready to go to the toilet, the brain sends messages via the nerve pathways to the bladder muscle and sphincter. It coordinates the contracting of the bladder muscle with the relaxation of the sphincter muscle. This discharges urine from the body.
How spina bifida affects the urinary system
A person with spina bifida is usually born with an anatomically normal urinary system, however, because the nerves in the lower lumbar and sacral region in the spine don’t form properly in spina bifida, most children have a condition known as neurogenic bladder. This causes incontinence, where there can be either partial or complete loss of voluntary urination. Nerve damage can result in impairment to the muscles of one or more of the following areas: the bladder, the urethral sphincter, or the flap attached to the ureter.
The neurogenic bladder can be either spastic or flaccid.
- A spastic bladder continually squeezes and therefore does not store urine. The muscles that line this type of bladder are extremely sensitive and irritable. They contract in a disorganised way and expel urine immediately after it enters the bladder. Even though the bladder is continually contracting, some urine almost always remains in the bladder.
- A flaccid bladder is one where the muscles are limp, and cannot contract completely to force the urine out. When the flaccid bladder becomes full, excess urine spills over and flows out of the body through the urethra. Urine dribbles out continually and when excess pressure is put on the bladder such as when laughing or crying this dribbling becomes more severe. However, the bladder never empties completely and some residual urine always remains.
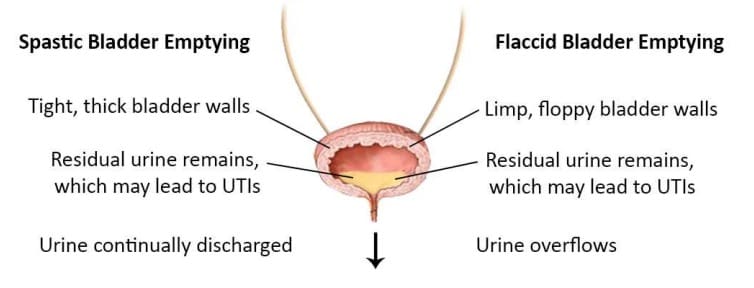
Diagram of urine flow of a spastic or flaccid bladder with normal or low sphincter tone
The bladder is also influenced by the control of the urethral sphincters. Where nerve damage exists, the sphincter muscles can be either too loose or too tight. If the sphincter muscles are too loose, urine continually leaks out of the body (as above). When the sphincter muscles are tight, urine becomes trapped in the bladder and is often forced back up the ureters to the kidneys. This is known as reflux.
The urine, which refluxes back up to the kidneys, can be very damaging to the whole urinary system, but especially the kidneys. Normally, muscular flaps on the ureters close and once the urine flows out of the kidneys, it cannot flow back. However, the muscles that control these flaps are often damaged with spina bifida, and instead of urine following the path from the kidneys to the bladder and outside of the body, the urine can flow back up the ureters to the kidneys.
It is very important for a person’s health that the bladder is completely emptied regularly. Urine that remains in the bladder provides an excellent breeding ground for bacteria, which thrive in warm, damp conditions. Repeated, severe infections in the bladder and urinary tract, over time, substantially damage the kidneys and impair their filtering capabilities.
The signs of a urinary tract infection, or UTI, include:
- cloudy or discoloured urine
- strong smelling urine
- blood in urine
- fever, chills and shakes
- headache, fatigue
- decreased appetite, nausea & vomiting
- pain with urination (burning or stinging)
- an increased frequency and need to urinate, or episodes of wetting between catheters if normally dry.
A person with spina bifida who has impaired function in the lower extremities should monitor the appearance of their urine carefully since they may not be able to feel the first warning signs of a urinary tract infection, such as pain while urinating.
Children, who have the most severe type of spina bifida (myelomeningocele), will almost always be affected by urinary incontinence. However incontinence is not limited to these children. Children with the milder types of spina bifida (occulta, lipoma, and meningocele) or similar neurological conditions may also experience similar difficulties to varying degrees.
How is my child’s urinary system functioning?
There are a number of medical investigations or tests your child’s G.P., paediatrician or urologist may order from time to time to monitor the health and functioning of the urinary system. These are some of the tests commonly used:
Routine Urine Examination
Freshly voided urine is examined under microscope for any signs of infection (bacteria, pus cells), bleeding (red blood cells), crystals (stones) or casts (nephritis). A chemical analysis is also done to check kidney function.
Renal Ultrasound
Shows how the kidney looks and if there is any swelling, pus collection, stones or other problems. It also gives information about bladder wall thickening and health of the ureters.
DMSA Scan
This scan is done to checks for signs of infection in the kidneys or to look for any scarring of the kidney post infections. This test also gives a very precise idea about the relative kidney function on either side.
Micturating Cystourethrogram (MCU) or Voiding Cystourethrogram (VCUG):
A catheter is placed into the bladder. A dye that can be seen on X-rays is instilled into the bladder through the catheter. X-ray images are obtained during filling and urination. A healthy bladder appears smooth. A neurogenic bladder often shows ‘out pouchings’.
Urodynamic Studies
The urodynamics study is a series of tests used to assess how well your child’s bladder and urethral sphincter are doing their jobs of collecting, holding and releasing urine. The main test involves a thin, flexible tube (catheter) being inserted into the child’s bladder to fill it slowly with a warm saltwater solution. At the same time, bladder pressures are monitored and the presence or absence of premature bladder contractions is noted, along with any sensations experienced by your child.
What are some management techniques?
There are three main aims of bladder management:
- Prevention of reflux of urine to the kidneys
- A reduction of urinary tract infections
- Achieving social continence
Due to the nature of the neurogenic bladder, most children with spina bifida will never achieve total control of their bladder and urethral sphincter to void urine ‘normally’. What most children can achieve, however, is social continence. Children achieve social continence by learning techniques that will help them to stay dry throughout the day and night, and to have back-up plans for accidents. The techniques are quite discreet and only those people close to them need to know.
To become socially continent one or more of the following strategies may be used. These strategies may not always work the first time, and you may need time and patience to find 10 SBH Queensland the right method for your child. Remember, not all techniques suit all children and the same child may need different techniques at different times.
1. Clean Intermittent Catheterisation (CIC)
Clean Intermittent Catheterisation (CIC) is one of the main techniques used. The bladder is completely drained every 3-4 hours throughout the day with a clean (but non-sterile) catheter. It is a relatively simple skill which children are encouraged to become independent with from an early age.
2. Medication
Different types of medication are prescribed for different reasons. Some medications may relax the bladder walls to allow for greater retention. Some help to dry up the bladder and some are important in clearing and reducing the occurrence of urinary tract infections. As with any medication there may be side effects. Find out what these may be when any medication is prescribed. If you are unsure why your child is on a particular type of medication, ask!
3. Adaptive Clothing
Whether your child walks or uses a wheelchair, and to what degree he or she is bowel and bladder incontinent, will determine whether adapted clothing would be of benefit for your child. If adaptive clothing is required you can then decide which range of products would best suit your child’s needs. Over the years, some items of clothing have been found to work better than others by parents who have ‘been there, done that’. For instance, pants with a Velcro front make dressing and undressing for toileting much easier, quicker, and allow greater independence.
4. Incontinence products
Incontinence products are available either through your local supermarket, chemist or online suppliers (e.g. Independence Australia or InTouch). Continence aids can also be subsidised through the CAPS or MASS schemes, which will be covered later in the booklet. Products include items such as pads, liners, nappies, pull-ups and catheters.
5. Toilet timing
As with many children without spina bifida, bladder management can be all in the timing. As your child grows older, your paediatrician, stomal therapist, or occupational therapist may discuss timed toileting with you as an option to maintain continence and health.
6. Behavioural Strategies
Toileting time is not always the most exciting time in children’s lives. As a great deal of focus may be put into this private part of their lives, it is always important to remember to encourage them and foster a sense of achievement by using behavioural strategies such as sticker charts and positive reinforcement.
7. Possible operations
As always, there are surgical procedures that may be suggested when other techniques are not sufficient.
- Bladder Augmentation – A surgical operation where a section of the bowel (usually) is cut away and sewn onto a surgical opening in the bladder to create a large bladder with increased capacity.
- Inserting an Artificial Urinary Sphincter – A surgical procedure whereby a small fluid filled cuff is placed around the neck of the urethra. A pump is also inserted which when activated, releases the pressure off the cuff, allowing urine to flow.
- Mitrofanoff – An opening in the lower abdominal region near or in the belly button is created using the appendix or a piece of small intestine that is made into a tube. This allows for easy access to the bladder directly for catheterisation. Named after Professor Mitrofanoff, who pioneered the procedure, also known as an appendicovesicostomy.
- Vesicostomy – An opening is created in the abdominal wall, below the undies line, that allows urine to drain continuously from the bladder into the child’s nappy or pull-up. This procedure is usually done to protect the kidneys when they are at high risk of damage, such as when the child has a very tight urethral sphincter. More information on each specific operation is available and should be discussed in detail with your urologist and/or paediatric surgeon.
8. Regular check-ups
It is important to remember that even after a child has begun their independence training, they will need to see the appropriate doctors regularly to monitor kidney and bladder function. It is through these regular check-ups that the doctors can monitor any slight changes in appearance and function, and therefore treat by prevention rather than cure.
Of course the most important thing to encourage a child to do to keep their bladder and kidneys clean and healthy is to drink plenty of water. This is often easier said than done. But, persistence is important, as it may just be what their kidneys need!
The bowel
The human body is designed to rid itself of waste products. If we do not rid ourselves of these waste materials we can become very ill. The organs that help our body expel waste are part of the lower digestive system, and are known as the intestines, or ‘bowels’.
How does the bowel system work?
The main parts of the bowel are:
Small intestine
A long narrow tube in which many secretions from different organs of the body, such as the liver and pancreas, are sent to break down the products moving through it. Nutrients are absorbed and the remaining undigested materials are transported to the large intestine by a series of waves of muscular contractions that squeeze the contents along, called ‘peristalsis’. Backflow of materials from the large intestine is prohibited by a muscular flap; much like urine is prohibited from going back up to the kidneys from the bladder.
Large intestine (Colon)
Most of the digestion has already taken place by the time the matter reaches the large intestine. The main functions of the bowel are to absorb water and electrolytes from the remaining materials, as well as to form, store and expel the faeces from the body. At regular, uncontrolled intervals these materials are pushed down from the large intestine into the rectum by peristalsis.
Rectum
The rectum is the last part of the large intestine. Its main purpose is to transport faeces to the anal canal to be expelled, and to store faeces when the brain dictates that a bowel movement is not appropriate at the given time.
Anal Canal
The anal canal is a short section of bowel that joins the rectum and the anus, and is surrounded by two sphincter muscles, the internal sphincter and external sphincter. The internal sphincter senses when faeces in the rectum and relaxes so that its lining can detect whether the matter to be passed is gas, liquid or solid. Nerves located in the anal canal send a message to the brain that a bowel movement is required. The bowel movement does not occur automatically at that particular time because of the external sphincter, a muscle we usually learn to control in the early years of life. When it is convenient, such as when we are sitting on the toilet, this muscle relaxes, and a combination of rectal contractions and tightening of the abdominal muscles, pushes the faeces out of the body.
Bowel continence
The human body is designed to rid itself of waste products. If we do not rid ourselves of waste material we can become very ill. The organs which help our body cleanse itself of waste are part of the lower digestive system and are often called the ‘bowels’.
How the bowel system works
The bowel consists of the small intestine, the large intestine, the rectum, internal and external anal sphincters and the anal canal. The large intestine (the colon) stores the waste material in liquid form and moves it along towards the rectum by a series of waves and contractions known as peristalsis. While the faeces is in the colon, excess water is removed from it until it forms the consistency of a stool. The internal anal sphincter located below the rectum, opens automatically when it senses that there are faeces in the rectum. Nerves located in the anal canal send a message to the brain that a bowel movement is required. When it is convenient the brain tells the external sphincter to relax and the rectum and the stomach muscles to contract. The faeces is then discharged from the body. We usually learn to control this process between the ages of one and three.
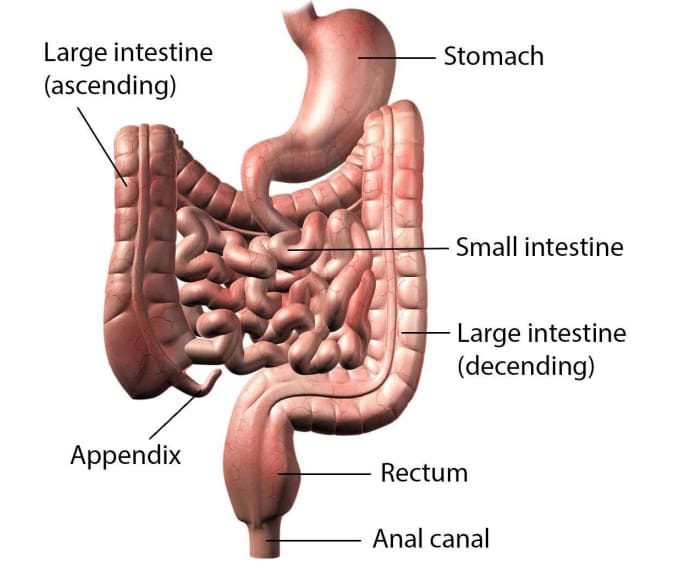
Normal bowel anatomy
How does spina bifida affect the bowel
Almost all people with spina bifida have some form of bowel incontinence. However, the degree and type of incontinence varies from person to person. As with most of the conditions associated with spina bifida, bowel problems are a result of damaged nerve pathways, therefore the child may be described as having a neurogenic bowel. The nerves that control and provide sensory feedback from the bowel exit the spinal cord at the sacrum (S2-S4). Nerve damage generally affects:
- The speed that faecal matter moves through the bowel (known as gut motility)
- The mechanism that alerts the child that the rectum is full
- The two sphincter muscles
- The muscles that assist the bowel in expelling faeces.
Motility
As mentioned earlier, in the normally functioning bowel, the waste products are moved through the bowel towards the anus by a series of muscular contractions that squeeze, like squeezing a toothpaste tube. These contractions are automatic and spontaneous. In the bowel of someone with spina bifida, the movement is generally a lot slower, which leads to constipation (hard stools).
Nerve damage
Nerve damage may affect the child’s ability to realise when the rectum is full in two ways. The first is a limited sensation of what is happening in the bowel and the second is a decreased ability to alert the brain to empty the rectum. Therefore, when the rectum is full the child doesn’t recognise the need to go, and accidents result because the child remains involved in the present activity rather than finding a toilet.
Sphincter control
In a typically functioning bowel, the person can control the external sphincter to hold the faeces in the anal canal, and push stools back to the rectum for temporary storage. However, because a person with spina bifida often has little or no control over the external anal sphincter, it is often loose and faeces can be forced out of the body at an inappropriate time.
Muscle control
Typically, when it is time for a bowel motion, the faeces are pushed out of the body by peristalis in combination with the pelvic floor muscles, the abdominals (“abs”/tummy muscles) and the diaphragm (the large muscle under your lungs for breathing). For children with spina bifida, control of the pelvic floor muscles is often impaired, and the peristalsis is slower than usual. Therefore the abdominal muscles and diaphragm are the main muscles used to assist with passing faeces. Sometimes these muscles are also weak.
Without implementation of a good management plan, having neurogenic bowel can lead to a series of problems such as constipation, impaction (an immobile build-up of faeces in the rectum), or rectal prolapse (where part of the bowel wall falls down through the anus).
Constipation occurs when the stool is unable to be removed from the body and becomes hardened because the water it contains is absorbed back into the body. Being constipated can make a person feel nauseated, grouchy, and generally very sick.
How is my child’s bowel functioning?
In order to assess bowel function, the following medical investigations are used by G.P.s, Paediatricians and Specialists:
- Physical Examination: Doctors often palpate (gently press) the abdomen to feel for the presence of faecal impaction.
- Bowel Diary: You and your child may be asked to keep a record of the child’s bowel movements for a week or two.
- X-ray of the abdomen: The X-ray picture can show the faeces in the bowel. If a buildup of faeces is detected (faecal impaction) the doctor or nurse will make a plan to clear the blockage. If the build-up is allowed to continue, a megacolon may develop, which involves the bowel becoming over-stretched and the bowel walls thinning.
What are some management techniques?
The important aims for bowel management are for the child to:
- Establish regular bowel evacuations. This reduces incontinence and the risk of a megacolon developing.
- Achieve social continence with independence and confidence in their bowel management strategies.
As with the bladder, management of the bowel is often an ongoing issue throughout the child’s life. Different combinations of strategies may be tried to achieve the best option for your child.
Good Bowel Routines + More Effective and Predictable Emptying = Social Continence
Some management techniques that may be suggested include:
- Toilet training and timing is similar to timed toileting for the bladder, where regularity is the key. It is an important part of starting a routine with your child, and will be very specific to his or her needs. It may involve different techniques such as bearing down, perhaps by laughing and coughing, to help the pushing. This should be done a certain number of times during the day and at regular times. It may also include regular enemas to ensure a clean day at school.
- Medications and supplements are often given to change the consistency of the faecal mass moving through the child’s bowel. A certain consistency is required for the faeces to be pushed out whether this is done voluntarily or involuntarily. Medications and supplements may add bulk to the faeces, stimulate the bowel movements, or slow the bowel movements down. Again, the specialist will look at these depending upon the individual circumstances of the child.
- Nappies/Incontinence Pads/Pull-Ups are used by young children, and children who have unpredictable emptying of their bowel, regularly. These products contain the mess of a bowel accident until the child can get cleaned up. Our aim is for families to develop a 15 SBH Queensland bowel management plan that consistently avoids unplanned emptying of the bowel so that children can progress to wearing undies.
- Enemas and Bowel Washouts will be recommended by the doctor or specialist in specific combinations and frequency. They may be used either through a stoma (e.g. M.A.C.E., see below), or through the anal canal (such as the Peristeen system). Both techniques involve longer than usual periods of time on the toilet for the child to allow for a full clean out.
- Behavioural strategies: Sitting on the toilet for long periods of time is not exciting for children who want to play. Behavioural strategies may need to be used to occupy them with something else, teach them how important this is for them, and to use the time effectively. Some children finish off homework while on the toilet, play with a Nintendo or iPad, or even watch television while waiting on the toilet.
- Anal plugs are often helpful in situations such as swimming lessons or day outings where social continence is a high priority. These are generally not recommended as a means of regular continence management. You should discuss these with your urologist, stomal therapist or occupational therapist before using them.
- Manual Evacuation (Gloving) is often used in conjunction with pushing, to help the faeces exit through the anus, and to ensure a greater evacuation. It involves either the carer or the child manually evacuating the bowel using their finger.
- Diet is a very important area for all children and should always be considered in conjunction with any other techniques. The following page contains a list of handy hints to consider regarding the diet of your child. Please speak with your doctor and dietician at your hospital when formulating new diets.
- Exercise: Many children with spina bifida, due to mobility difficulties, or lack of motivation, are not as active as other children. Regular exercise and increased movements are not only beneficial for the child’s strength, health and size, but are also very important for helping to maintain a healthy bowel by improving gut motility.
- Possible Operations: When more conservative measures are insufficient for achieving social continence and independence, a surgical procedure may be suggested. More information is available on this from SBH Queensland and your hospital. Remember to ask your urologist many questions before deciding.
- M.A.C.E. (Malone Antegrade Colonic Enema, or Appendicostomy): The M.A.C.E. (or A.C.E) involves the creation of a stoma (opening) for easy access into the large bowel in order to irrigate (wash out) the bowel. The appendix is often used as the duct between the opening and the bowel.
- Chait Trap door (Cecostomy): Works in a similar way to a MACE for bowel irrigation. A small tube is inserted from the outside of the body into the cecum (beginning of the large intestine, near the appendix).
- Regular check-ups with the urologist and paediatrician will help to maintain a healthy bowel.
Handy hints for diets for your child with Spina bifida
One of the most practical and important lessons you can teach a child about food is that the amount of food going in must equal the amount of energy being put out by them. If your child is putting on excessive weight, look at the amount and type of food they are eating.
Often, the best diet for youngsters is generally to eat whatever their parents eat. This means that if you typically have a reasonably well balanced diet with minimal junk food, then this is a good place to start when creating your child’s diet.
Some ideas to think about and discuss with your doctor and dietician:
- Adding or reducing fibre in the diet will change the consistency of the child’s stools. This can be done using different foods or supplements in a tablet or drink form. Different types of fibre have different impacts, so check with your dietician if you have any concerns.
- Adding or reducing fruit and fruit juices can change the consistency of the stools. Make sure you watch for intolerances to some fruit sugars as this may cause loose stools. The most popular fruits for loosening up stools for more regular movements are prunes, apples and pears (as well as apple and pear juice), cranberry juice, nuts, apricots, pineapples, melons, oranges and sultanas. Of course, fresh fruit with the skin on is higher in fibre than something that has been peeled or tinned, so keep the skin on your apples, pears, apricots and grapes!
- Vegetables are very good for the bowel. Cabbage, corn, Brussels sprouts, cauliflower, peas, beans, carrots (uncooked especially), and celery are all good for keeping the stools a smoother consistency. (Some vegetables, such as cabbage, may cause increased wind, and consequently should be watched carefully.)
- New foods should be introduced by adding small quantities to the food the child routinely eats. For example two or three peas with the mashed potato. This will let you know firstly, if they like it, and secondly, whether it will have any effect on their system.
- Foods with high amounts of carbohydrates such as breads, potatoes and cereals will help bulk up the amount of stool and avoid loose messy stools. They also provide lots of energy to burn, which is important for all children. Remember though to balance the input and output so children are neither over-filled and putting on weight, nor underfilled and losing energy.
- Diarrhoea can be caused by certain ‘trigger’ foods. Common triggers include chocolate, foods with high sugar content, greasy foods, and spicy foods. If loose stools are a problem, trial eliminating these potential offenders from the family diet.
- Many families have found positive effects from using probiotics, such as Yakult or Inner Health Plus. As you may imagine, an enema will not only wash out the unwanted faeces from the bowel, but may also wash out a lot of the good bacteria as well. Research has shown that taking a probiotic may prevent diarrhoea associated with taking antibiotics and help with maintaining general health.
- Research has shown that taking cranberry juice every day increases the ability of the bladder to defend itself against bacteria. It appears that the cranberry juice helps the bladder’s immune system by stopping the bacteria adhering to the bladder wall.
We are constantly on the lookout for any more good dietary suggestions, so if you happen to come across any good ideas yourself, please let us know so that we can pass them on to other parents.
Most importantly, don’t try to rush. Finding the perfect diet can take time, and unfortunately it may also change. What seems perfect at one time may not be suitable twelve months later.
Handy hints for exercise
Exercise is an essential part of a healthy lifestyle, and it’s important that every member of the family can participate. Many children with spina bifida are not as active as their peers. This can be due to either their physical limitations or lack of enthusiasm for active play. It is important for children with spina bifida to maintain a healthy weight and in turn, to maintain their mobility and strength. Remember prevention is better (and often easier) than cure.
Physical benefits of exercise:
- Continued development of fine and gross motor skills
- Improved balance, coordination, rhythm and timing
- Improved bilateral skills, symmetry
- Improved motor planning, body awareness and spatial awareness
- Increased fitness
- Improved health and body function
Psychological benefits of exercise:
- Improved self-esteem and self-image
- Increased motivation to move
- Forming social connections
- Improved mood and attitude
Incontinence can be an issue during physical activity, as movement helps the bowel work. Therefore, it’s important to plan ahead and set-up good routines around exercise to ensure a fun experience and reduce anxiety related to the possibility of having an accident.
To tip for preventing accidents during exercise
Empty the bowels prior to the exercise, using your child’s usual methods, either the night before, or the morning of, special events like school cross country or sports carnival. Then, immediately before the event, encourage the child to sit on the toilet and push, rock, cough or laugh to empty any remnants. It might still be wise to use back-up, such as a pull-up, during the event.
Recommended forms of exercise for children with Spina bifida
Of course, children should be encouraged to pursue their own interests so long as the activity is safe. Getting moving is easy! You could start with a walk or wheel around, go swimming, or join you local gym. There are lots of sports and recreational activities available for people with disabilities. Ask your Physiotherapist to find out what is available in your area.
Can a child with incontinence go swimming?
Yes, many children with spina bifida regularly attend swimming lessons and have found swimming an excellent way to improve both fitness and strength. However, there are a few things that need consideration before attending the pool.
Is there likely to be an accident in the pool?
Do not assume that because the child has spina bifida or because they are bowel incontinent that they will have an accident in the pool. Preparation can be done before hand, at home in the morning or just before entering the pool, to ensure the child has an accident-free day in the pool.
Will the child be compliant?
It is very important to ask your child if he or she wants to participate in the swimming program, and whether he or she agrees with the bowel management strategy to be used for this activity. This is particularly important for those children who may have to use temporary strategies to remain accident free in the pool.
Preparation at home simply involves the everyday routine done for an accident free day at school, such as an enema, bowel washout, or timed toileting with medications.
Other temporary management strategies include:
Disposable Swim Nappies: For small children, swim nappies, such as Huggies “Little Swimmers” or Aldi’s “Mamia” swim nappies are a popular and effective choice.
Anal Plugs: These are small, soft plugs, which are inserted much like a tampon into the anus, and are able to stay there for up to 12 hours. They will keep the child completely accident free during that time. Research on use of anal plugs by children with spina bifida suggests that the larger size is preferred by most.
Washable Incontinence Swimwear: For older children, reusable swimwear can be chosen to contain any bowel accidents, and can be very discreet, such as the options pictured below. These options are available for purchase online.
Self esteem and independence
Toileting is one of many life skills that the child will need to master, and any problems with it can have a big impact on self-esteem. Therefore, it is not simply treated with a short burst of intensive training. The entire process may take a long time to master successfully, many years in some cases. The SBH Queensland team regularly monitor children’s progress with toilet training and particularly target skills such as regular clean intermittent self-catheterisation.
Self esteem is a very important issue closely connected with toileting and continence. It is easily affected by the way these issues are managed. Decisions on toileting routines both at home and at school, must be made in the context of the child’s self esteem. Plans should therefore be made in conjunction with your child about his or her own toileting program. All routines should consider what is expected of the child, what happens if there is an accident, who can they talk to about this, and what back up plans can maintain privacy. A rule of thumb, to minimise embarrassment to the child and to maintain a respect for privacy, is to take a no-fuss, objective approach.
When to begin independence training will depend on what management strategies are being used. Training for bladder management, such as catheterisation, is commonly begun by preschool age, beginning with the background steps such as hand washing, undressing and dressing. By this age these are usually quite easy for a child. The speed with which you progress through independence training will be determined by how quickly and easily your child is able to achieve each step. To become independent, your child must learn steps including:
- personal hygiene,
- dressing and undressing,
- transferring onto and off the toilet or change table,
- management of any accessories required (pads, catheters, etc),
- correct sequencing of events, and
- correct timing.
Independence in the management and health of their own bowel and bladder is a big responsibility for a young child, and should not be rushed.
During the first few years at school, children with spina bifida usually require assistance at first, and then supervision of continence management. Occupational therapists can help you in this area, as well as provide information and guidance to those involved when required. Checklists, sequencing picture cards, and motivational charts are often used, depending on what appeals to each individual child. Consistency of routine between the home and school is very important for the child to gain and maintain steps to independence.
It is also very important to consider the environment in which independence training is to be taught and followed through. Toilets and bathrooms must be accessible for children whether or not they use a wheelchair. For example, a sink, which is too high for the child to reach properly, compromises the hygiene steps. An occupational therapist can also assist you with the accessibility of toilets, bathrooms and all settings.
Teaching children about themselves is also an important step towards independence. This includes understanding the anatomy of the body (using a mirror), the effect spina bifida has on the body, and the reason it is important to follow the toileting program.
Finally, it is important to remember that many children with spina bifida experience regular periods in hospital, or in plaster or in splints. Independence training may be halted or may even take a small step backwards during this period. Patience will be needed to work through these delays, and great encouragement and praise must be given when new skills are acquired.
Compliance
A very important thing to remember as a parent is that all children go through a stage of non-compliance at one time or another, where they avoid completing their toileting plan. Quite often this is related to the child wanting to feel, be, and do the same as their peers. This may range from simply becoming totally involved in an activity and forgetting to go, to being sick of toileting differently to others and to not wanting to do the routine at all anymore. However this happens, the length of time this lasts will depend on how it is handled.
- Being consistent and having good communication among all involved will enable you to see if problems are occurring at either home or school, and help to resolve them quickly.
- Praise and rewards work very well for younger children when they begin their toilet training. They must be remembered for older teenage children also who because they have become independent will not have the same amount of adult contact time as they previously did.
- Bargains and contracts can be used with children to help them to remember and complete their routines. One good strategy used for a child who constantly forgets the time for toileting may be to have a small beeper or alarm set on their watch to remind them.
Compliance is an important issue to address, as it not only challenges the patience of the family and school, but will also affect the health and well being of the child.